Sam S.
-
Posts
213 -
Joined
-
Last visited
Content Type
Forums
Events
Gallery
Everything posted by Sam S.
-
Thanks for posting! I'm about 3 hours away, but as I was looking over the list can't imagine how I'd haul everything else (besides the KP-301's) in that auction away. 2 plasma TV's and that massive whiteboard. They probably would've done better separating those things out. Who knows, maybe it'll ultimately go cheap and be worth hauling the other stuff off. I did note the ad said KP-301, but the pictures clearly show KP-301 ii.
-
The perfect integrated doesn’t exist…and it’s annoying
Sam S. replied to CoryGillmore's topic in Solid State
Good luck. PrimaLuna 200, 300, or 400 all have HT bypass. I found my e-mail from Mark @ Rogue from Jan, 2021. At that time, the Cronus Magnum III or Sphinx could add HT bypass for an extra $150. Might be worth consideration as price-wise that'd be in the same category or less than the PL200. Rogue made in US and Primaluna China if that matters to you. Another consideration might be the Rogue Pharoah (tube pre-amp and SS amp) which comes standard with HT bypass. Specs here. Pharoah (just on the high side price wise from the PL200) would have way more power than your CW's would require. -
The perfect integrated doesn’t exist…and it’s annoying
Sam S. replied to CoryGillmore's topic in Solid State
Few suggestions --- Have you considered offerings from Rogue -- either the Cronus Magnum or the Sphinx? I don't think they come standard with HT bypass, but when I was looking a year or so ago and considered HT bypass to be something I wanted, I emailed them and it was available as an option to add for like $100 or $200 more. I'd think either would pair well with the CW's. Or for a more pricey option, the McIntosh MA352 has a HT bypass. I realize this may start a tubes v.s. solid state debate, but you didn't specify in your post, only asking for the "perfect integrated". Such a thing may not exist. I'm assuming your post is asking for suggestions for an integrated to play 2-channel sources through the CW's, but with the bypass for an AVR since the CW's do double duty for HT? Also - as Fido mentioned, some of the PrimaLuna's also have HT bypass. Might be worth a look. -
Thanks, The Dude. I've thought about that. I believe it's a 2x4. I think if I cut the hole for the speaker, I can look up in there to see for sure. Plan B could be carefully taking off the baseboard and running it down underneath. I just wanted to make sure I wasn't missing anything in the planning stage.
-
Hi -- Seemingly a basic question I'm struggling with. I recently scored some free in wall speakers and want to add these to the sides in my basement. One side of the room is no problem, as the wall backs to a utility area that has easy access. The other side is more problematic, but I have access to the ceiling joist opening from the utility area, but here's my question---If I open the area to put the in wall speaker in, what is the best way to run the wire. I know I can run it down, and then under the baseboards, but then I'd have to carefully take these off, and hopefully not re-paint afterwards. Going up the wall and then across the joists makes more sense, but it looks like there's a header at the top, so that appears to be a roadblock. How do people typically run this? Thanks!
-
The Economist analyzed existing data and used it in generating a COVID risk calculator. Of course, this doesn't assess your risk of catching COVID, but assuming you were infected, it allows you to enter your age, and any other conditions and determine what the projected outcome might be (it also doesn't consider potential long term tissue damage from COVID). For instance, a 25 year old female with no preexisting conditions has a risk of hospitalization of 1%, and risk of death of .1%. By comparison, a 70 year old male with hypertension, type 2 diabetes, and who is obese has a risk of hospitalization of 38.3% and risk of death is 6.7%. Here's the tool: https://www.economist.com/graphic-detail/covid-pandemic-mortality-risk-estimator To the other point about vaccine records and school requirements, those vaccines (MMR etc) are, technologically speaking, widely different than the existing Covid vaccines. The other vaccines, which have been in use for many years and thus have years of use data, use a live, weakened virus. The technology in the AZ/J&J vaccines use a similar delivery method (weakened adenovirus) to deliver double stranded DNA, of which the goal is then the spike protein. So the new technology (DNA - spike protein) and the older more widely used delivery method. The Pfizer/Moderna vaccines use 2 new technologies - the delivery method (lipid nanoparticles) to deliver the mRNA (which also targets the spike protein). The point is comparing MMR vaccines to COVID vaccines is like comparing apples to oranges so to speak, aside from any debate about short and long term effects of either.
-
Interesting if you look at the positive case data from that dashboard for Texas from May of 2021 and compare that to May of 2022: 5/5/2020 - 1.1K cases v.s. 5/5/2021 - 1.8K cases 5/11/2020 - 1K cases v.s. 5/11/2021 - 2.9K cases 5/20/2020 - 1.4K cases v.s. 5/18/2021 - 2.8K cases 5/25/2020 - 1.9K cases (same as 5/25/2021)
-
Someone asked about COVID comorbidities, or conditions contributing to COVID deaths. The CDC publishes those data. As of 5/2/21, 1,548,610 conditions contributing to death were listed in addition to COVID (560,616). You can also view those data by age group, state, etc. For those curious, here's the list: Condition COVID-19 Deaths Influenza and pneumonia 257,022 Chronic lower respiratory diseases 49,659 Adult respiratory distress syndrome 58,537 Respiratory failure 210,769 Respiratory arrest 11,866 Other diseases of the respiratory system 23,427 Hypertensive diseases 110,763 Ischemic heart disease 61,327 Cardiac arrest 68,105 Cardiac arrhythmia 41,680 Heart failure 42,831 Cerebrovascular diseases 27,788 Other diseases of the circulatory system 35,720 Sepsis 53,604 Malignant neoplasms 26,525 Diabetes 89,748 Obesity 22,204 Alzheimer disease 20,411 Vascular and unspecified dementia 55,189 Renal failure 55,849 Intentional and unintentional injury, poisoning, and other adverse events 11,227 All other conditions and causes (residual) 214,359 COVID-19 560,616
-
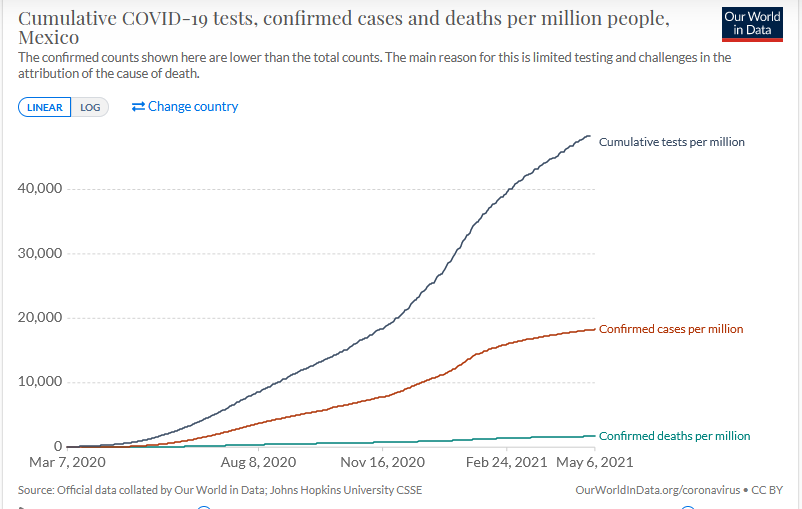
Similar to the U.S. chart, but a higher increase in confirmed cases. In the U.S., cases are roughly double what they were about a year ago (45,000/M now v.s. about 24,000/M a year ago), but testing has also increased.

-
The original question was whether or not a wide range of differing expert or qualified opinions can contribute to the topics debatable around COVID (thinking broadly about this). Your response clarified that to mean only "top scientists" should be listened to and then you clarified that further (narrowly) to the CDC and WHO. It seems appropriate to include others with research and experience in virology, epidemiology, infectious diseases, evolutionary biology...should if they choose have a voice and as the original poster suggested, and participate in an honest debate about issues. We have nowhere near that. We have a handful of individuals who have constructed a series of narratives and anyone who disagrees or even questions that narrative is attacked and labeled as a nutjob. This further obscures the issues, contributes to vaccine skepticism, and distrust among the general population. As for the WHO, this is part of it as the narrative pushed is that the lab leak hypothesis (I'm talking about lab leak, not a lab created then purposefully released) can't possibly be true. Many scientists have said that while they don't have direct evidence, they believe that a lab leak could explain a great deal about this virus. It should be noted that there is also no direct evidence of other narratives being pushed (e.g. wet markets, pangolins). There are many reasons for the lab leak theory. The most recent credibility issue with the WHO is that when they investigated these sorts of things, they weren't allowed to investigate anything on their own, but rather got information directly from the Chinese government, which concluded that it wasn't a lab leak (nothing to see here, folks). The WHO said "good enough", and didn't question it. There's good reason for them to lie or mislead about this (gov't). See NPR generally. The truth is at this time, we don't really know the origin. Finally, many certainly have an economic interest in the lab leak hypothesis to not be true. Those who've financially relied on gain of function research for grant and other funding. Evidence of a lab leak would certainly call that into question (because we sure as hell don't want this to ever happen again), and many that are vocal against any possibility of a lab leak stand to suffer financially if gain of function research is called into question.
-
Who gets to decide who the "top scientists" are and what criteria are used? Asking for a friend.
-
That's my point, the only articles are there to support the narrative of those that I mentioned, and Big Pharma, the "nothing to see here folks" narrative. What is the CDC doing to investigate these reports? Does the media actually talk to people who've had and reported these adverse events? Undoubtedly, some are quite minor, and others likely mis-reported or false, but all 100,000? You can't discount the narratives of people who describe their own actual experiences, especially when the clinical trials datasets are so (relatively) low.
-
Probably because adverse events really aren't investigated, and they certainly aren't reported in the media. Pharma and health "experts" have already been locked into the "safe and effective" narrative, so anything that runs contrary to that will be discounted as either outright false or an odd coincidence. According to the VAERS data, there were (as of this posting), 109,199 adverse events reported from COVID vaccines. I'd challenge anyone to find a mainstream news article that even mentions this. Instead, we see Scott Gottlieb, former FDA commissioner, plastered all over the news and talking about how everyone should vaccinate a 10 year old, with no mention of the fact that he is currently on the board directors for Pfizer, which stands to gain Billions in profits from vaccine distribution and repeated vaccinations.
-
Randy: Ivermectin has been approved by the FDA to be used as an anti-parasitic drug, and Billions of doses have been administered safely worldwide for years. The link you posted said it has been approved, but not specifically for COVID, so many doctors are using it off label as treatment for COVID. It's been used since the 70's, so it is now out of patent protection, which, to @oldtimer's point might be the reason Big Pharma might be opposing its use as they undoubtedly are trying to develop their own (patentable) drugs to treat COVID. There's no money to be made from Ivermectin. That's also likely the reason the media rarely if ever reports about it. The 2 doctors who discovered it were granted the Nobel Prize in Physiology and Medicine in 2015. Dr. John Campbell (who's been providing daily worldwide COVID updates and data), recently interviewed Dr. Pierre Kory about Ivermectin and it's use to treat COVID. Others have also completed research, including Tess Lawrie, who also was on Dr. Campbell's show. No one could call either of these guys quacks, or anti-vaxxers. It's an intelligent discussion lacking from today's landscape of one sentence sound bites.
-
Pfizer CEO has said (in leaked conference call) that he sees repeated vaccinations as a "great opportunity" to charge more for repeated vaccinations. For context, it's true that Pfizer didn't take money from "operation warp speed", but did use public funding from the German government. However,....mRNA research and development (like most pharmaceuticals) was researched and developed with public funding. Pfizer has claimed that the lipid nanoparticles that the mRNA is coated in are proprietary, and refusing to offer its technology to poor countries to produce vaccines that (according to health "experts" and politicians) could save lives. Not to mention the fact that the Pfizer vaccine is very narrowly targeted towards the specific spike protein, so if (or when) the virus mutates and further evolves, undoubtedly the original vaccine will begin to lose its effectiveness. This, for Pfizer, ensures repeat customers. Why aren't we having a proper adult conversation about how our health care system rewards and provides perverse incentives for chronic illness. Drug companies, insurance companies, and non-profit (tax-exempt) hospitals. How many times have we been urged or told we should get the vaccine? How many times any politician or health "expert" talk about obesity? 78% of all COVID hospitalizations in the U.S. are people who are either overweight or obese. You can also add opiods to the long list set forth by Carl above. There's good reason why many do not trust Big Pharma.
-
Not sure about the Avocet's, but you can't go wrong in my experience with Continentals. Maybe Michelin's or Vittoria's. I've mostly ran Continentals, super sport series tires, with good results. Offer decent bang for the buck, and generally very durable. As to your other questions, 700x23 if you are riding on the road (21's are too narrow and 19's way to narrow, and might not fit on your rims anyway). Number one cause (only cause) of pinch flats (snake bite as you say) is improper tire pressure (or maybe hitting a huge pothole, which will give you a flat no matter what). Make sure you have a good pump with a gauge, and check the pressure before EVERY ride (e.g. if they are rated 120 PSI max, run them at least 100 or more). If you happen to be riding on trails (e.g. limestone), then go with the 700x25's. You should be able to find decent durable tires for around $25-35 per tire, maybe less. If punctures are of concern, it might be beneficial to seek a kevlar belt, but even that's no guarantee against a puncture. Best to carry a spare tube, tire levers, pump or co2 if you aren't already. Good luck.
-
Interesting, as I have Chorus II's in my basement that are often unused, and looking to possibly try a different amp with them. The other thread OP started had a number of responses that seemed to indicate (as I've heard over and over again) that Chorus II's "need lots of power" and "pair best with SS". I'm not sure I buy that, but then again, I've not tried mine with tubes either. Nice to hear others have tried tubes and like the combo. I wonder why many say they pair well with SS? Seems to me a decent powered tube amp would sound rather nice. I have a Jolida/Black Ice F-22 upstairs (75 Wpc, El-34's) that sounds (to me) outstanding driving Forte III, and it seems as though the same result would apply to the Chorus II's, unless I'm missing something. One of these days, I'll get around to moving it down there for a test. OP - please report back on your experience after you get whatever you get. Here's the other thread for reference.
-
The stage 3 trials included 43,783 participants. They didn't disclose the sex or age breakdown, only that 34% were over age 60. https://www.jnj.com/johnson-johnson-covid-19-vaccine-authorized-by-u-s-fda-for-emergency-usefirst-single-shot-vaccine-in-fight-against-global-pandemic
-
Since the window of reported clots has been 9-14 days after the vaccine is given, many people are still within that window (e.g. say they just received their shot a few days ago), so we would expect those numbers to increase over the next two weeks. So far, it's women in the 18-48 demographic, but that was the same way the AZ data started, then later expanded to include men. The other thing to keep in mind here, is that in addition to the clotting cases reported, the J&J vaccine had 2 clinics last week (one in CO and one in NC) close because of immediate side effects and some being rushed to the ER for treatment. In addition to the reports of the J&J contamination (up to 62M doses) at the Emergent Bitsolutions manufacturing plant. I agree that the public health officials are doing the right thing, but.....aren't these sorts of data supposed to be uncovered in clinical trials?
-
Depends on how you assess risk and the data that are available, which is what they apparently are investigating now. The media is reporting the US cases affecting healthy women ages 18-48, so if you are in that demographic your risk likely would be much higher than say if you were a male age 74. However, IF the US data follows close to the AstraZeneca data in the UK, the first clot cases were reported were women, likely due to the fact that they were the first demographic to receive the vaccine (healthcare workers), and cases in men showed up later on as the data was collected. The risk analysis is a more complicated one - as you also have to factor in the risk of serious illness or death due to COVID. In other words, the risk to a healthy 20 year old woman likely would be different than a 76 year old man with multiple pre-existing conditions. I'm not sure, but I keep hearing that 6M number thrown out, and if that includes all J&J vaccines given to date we likely would see more blood clot cases over the next two weeks, as the others showed up between 9-14 days after given the vaccine (e.g. if someone was vaccinated last week, they wouldn't present with the clot symptoms until this week or next week). It's also important for the CDC and the FDA to get information to health care providers because it's my understanding that the typical treatment for these types of blood clots in people that have received the vaccine could likely have adverse effects, or kill them. Agree, that hopefully they can figure out what is going on. FYI - both the AZ and J&J shots use an adenovirus to deliver the DNA, but the J&J uses a human adenovirus (weakened), whereas the AZ vaccine uses one from a Chimpanzee.
-
"With all due modesty, I think I'm pretty effective." --Anthony Fauci, poolside Masks from the "store" don't "keep the virus out". --Anthony Fauci, Today Show Interview, also USA Today a month later Anthony Fauci has worn out his welcome We shouldn't expect people in the public health sphere to have all the answers, but don't pretend you do if you don't.
-
Exactly the point. If someone had maybe 10-20 years left (although it's hard to predict things) the weight of the risk/reward analysis might be completely different than say for a 5 year old, who has a much longer life expectancy.
-
Thanks for the link. Certainly, I agree that weighing the risk/reward and not only the short and long term effects of COVID is a very difficult decision for one to make. I was actually thinking about the Johnson and Johnson/AZ technology, which uses a new (not proven or tested long term) technology to deliver the double stranded DNA via an older, proven technology (weakened adenovirus), but the gist of those and the mRNA vaccines are similar, only the delivery device is different (lipid nanoparticles, which to my knowledge have never been used before (Pfizer/Moderna) v.s. the weakened adenovirus (Johnson and Johnson/AZ). The mRNA data cited in your article are for technologies that are still in clinical trials stage. AS your article states, no mRNA vaccines have ever before been approved for human use. Notwithstanding the delivery device being different (we don't know much about the lipid nanoparticles Pfizer is using because they are claiming it's "proprietary"), those other trials are in stage 1/2, whereas we are still waiting for Pfizer to release their stage 4 data.
-
Aside from the obvious response of whether or not someone should make a health decision based on what "POTUSAs, leading scientists [not sure what qualifies as "leading", I'm sure someone gets to decide who is and isn't based on their conclusion] business and societal leaders, etc", there are numerous examples of individuals in these groups that have expressed doubts or concerns about the vaccines. Some of it is suppressed in the media because it's off message (vaccine good, you take, you don't take you conspiracy theorist nutjob). Others, widely reported. Healthcare workers Politicians The debate or decision isn't simply "COVID v.s. Vaccine", you are making the vaccine decision based on the risk of COVID and other factors, which might include your age, health, pre-existing conditions, etc. Sort of like Russian Roulette, dangerous? Yes. Harmful? Maybe not - only in 20 some % of people that play it. Your argument (at least this one) is a classic "appeal to authority" (logically fallacious).